


 Sign Out
Sign Out



Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Patient Exposure: The data described in this section are derived from a clinical trial database consisting of a total of 3817 subjects (approximately 1705 patient-years exposure) with schizophrenia who received at least one dose of INVEGA SUSTENNA in the recommended dose range of 25 mg to 150 mg and a total of 510 subjects with schizophrenia who received placebo. Among the 3817 INVEGA SUSTENNA-treated subjects, 1293 received INVEGA SUSTENNA in four fixed-dose, double-blind, placebo-controlled trials (one 9-week and three 13-week studies), 849 received INVEGA SUSTENNA in the maintenance trial (median exposure 229 days during the initial 33-week open-label phase of this study, of whom 205 continued to receive INVEGA SUSTENNA during the double-blind placebo-controlled phase of this study [median exposure 171 days]), and 1675 received INVEGA SUSTENNA in five non-placebo controlled trials (three noninferiority active-comparator trials, one long-term open-label pharmacokinetic and safety study, and an injection site [deltoid-gluteal] cross-over trial). One of the 13-week studies included a 150 mg INVEGA SUSTENNA initiation dose followed by treatment with either 25 mg, 100 mg, or 150 mg every 4 weeks.
The safety of INVEGA SUSTENNA was also evaluated in a 15-month, long-term study comparing INVEGA SUSTENNA to selected oral antipsychotic therapies in adult subjects with schizophrenia. A total of 226 subjects received INVEGA SUSTENNA during the 15-month, open-label period of this study; 218 subjects received selected oral antipsychotic therapies. The safety of INVEGA SUSTENNA was similar to that seen in previous double-blind, placebo-controlled clinical trials in adult subjects with schizophrenia.
The safety of INVEGA SUSTENNA was also evaluated in a long-term study in adult subjects with schizoaffective disorder. A total of 667 subjects received INVEGA SUSTENNA during the initial 25-week open-label period of this study (median exposure 147 days); 164 subjects continued to receive INVEGA SUSTENNA during the 15 month double-blind placebo-controlled period of this study (median exposure 446 days). Adverse reactions that occurred more frequently in the INVEGA SUSTENNA than the placebo group (a 2% difference or more between groups) were weight increased, nasopharyngitis, headache, hyperprolactinemia, and pyrexia.
Adverse Reactions in Double-Blind, Placebo Controlled Clinical Trials: Commonly Observed Adverse Reactions: The most common (at least 5% in any INVEGA SUSTENNA group) and likely drug-related (adverse events for which the drug rate is at least twice the placebo rate) adverse reactions from the double-blind, placebo-controlled trials in subjects with schizophrenia were injection site reactions, somnolence/sedation, dizziness, akathisia, and extrapyramidal disorder. No occurrences of adverse events reached this threshold in the long-term double-blind, placebo-controlled study in subjects with schizoaffective disorder.
Discontinuation of Treatment Due to Adverse Events: The percentage of subjects who discontinued due to adverse events in the four fixed-dose, double-blind, placebo-controlled schizophrenia trials were similar for INVEGA SUSTENNA- and placebo-treated subjects.
The percentage of subjects who discontinued due to adverse events in the open-label period of the long-term study in subjects with schizoaffective disorder was 7.5%. During the double-blind, placebo-controlled period of that study, the percentages of subjects who discontinued due to adverse events were 5.5% and 1.8% in INVEGA SUSTENNA and placebo-treated subjects, respectively.
Dose-Related Adverse Reactions: Based on the pooled data from the four fixed-dose, double-blind, placebo-controlled trials in subjects with schizophrenia, among the adverse reactions that occurred with ≥ 2% incidence in the subjects treated with INVEGA SUSTENNA, only akathisia increased with dose. Hyperprolactinemia also exhibited a dose relationship, but did not occur at ≥ 2% incidence in INVEGA SUSTENNA-treated subjects from the four fixed-dose studies.
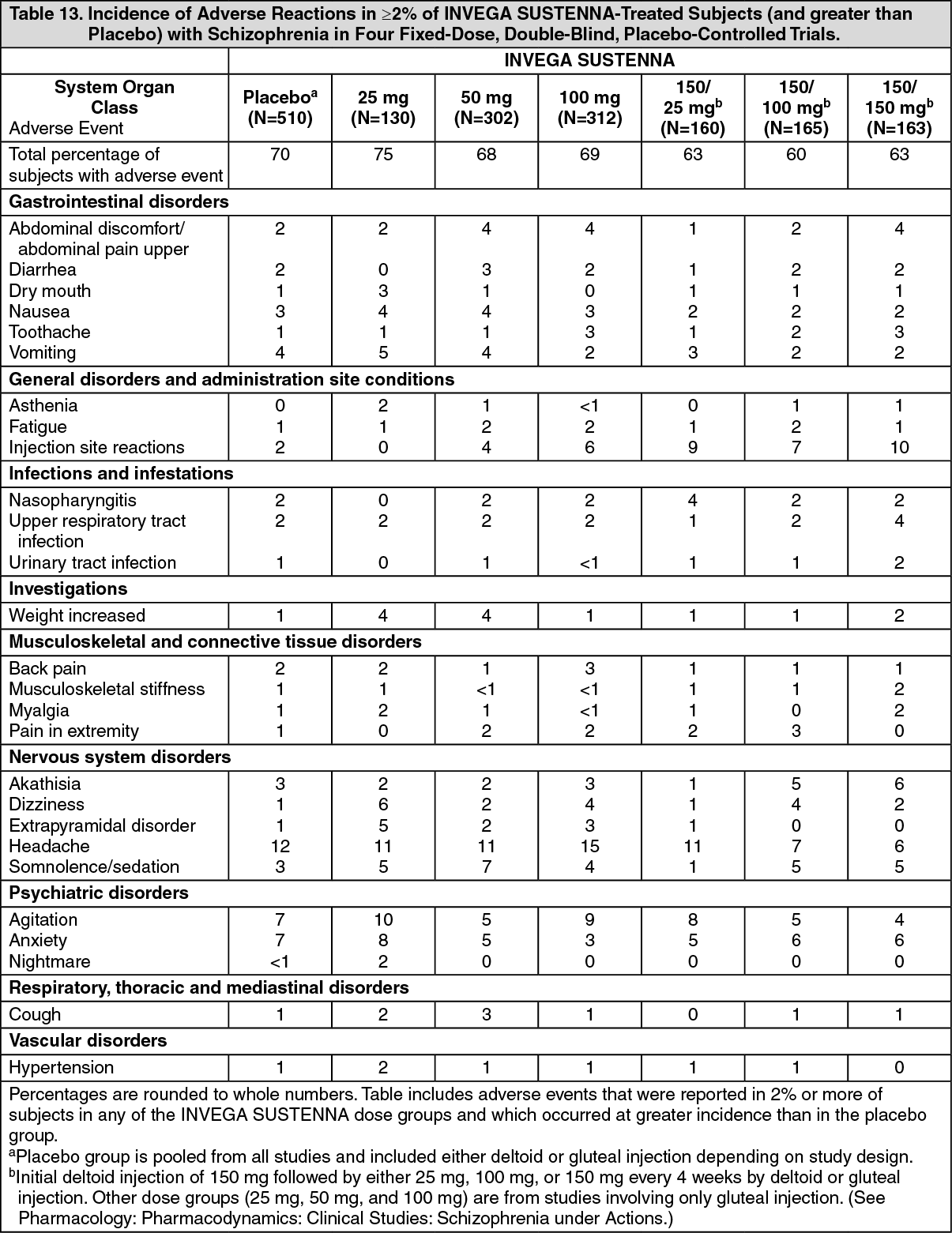
Adverse Reactions Occurring at an Incidence of 2% or More in INVEGA SUSTENNA Treated Patients: Table 13 lists the adverse reactions reported in 2% or more of INVEGA SUSTENNA-treated subjects and at a greater proportion than in the placebo group with schizophrenia in the four fixed-dose, double-blind, placebo-controlled trials. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdverse events for which the INVEGA SUSTENNA incidence was equal to or less than placebo are not listed in the table, but included the following: dyspepsia, psychotic disorder, schizophrenia, and tremor. The following terms were combined: somnolence/sedation, breast tenderness/breast pain, abdominal discomfort/abdominal pain upper/stomach discomfort, and tachycardia/sinus tachycardia/heart rate increased. All injection site reaction-related adverse events were collapsed and are grouped under "Injection site reactions".
Other Adverse Reactions Observed During the Clinical Trial Evaluation of INVEGA SUSTENNA: The following list does not include reactions: 1) already listed previously or as follows, 2) for which a drug cause was remote, 3) which were so general as to be uninformative, or 4) which were not considered to have significant clinical implications.
Cardiac disorders: atrioventricular block first degree, bradycardia, bundle branch block, palpitations, postural orthostatic tachycardia syndrome, tachycardia.
Ear and labyrinth disorders: vertigo.
Eye disorders: eye movement disorder, eye rolling, oculogyric crisis, vision blurred.
Gastrointestinal disorders: constipation, dyspepsia, flatulence, salivary hypersecretion.
Immune system disorders: hypersensitivity.
Investigations: alanine aminotransferase increased, aspartate aminotransferase increased, electrocardiogram abnormal.
Metabolism and nutrition disorders: decreased appetite, hyperinsulinemia, increased appetite.
Musculoskeletal and connective tissue disorders: arthralgia, joint stiffness, muscle rigidity, muscle spasms, muscle tightness, muscle twitching, nuchal rigidity.
Nervous system disorders: bradykinesia, cerebrovascular accident, cogwheel rigidity, convulsion, dizziness postural, drooling, dysarthria, dyskinesia, dystonia, hypertonia, lethargy, oromandibular dystonia, parkinsonism, psychomotor hyperactivity, syncope.
Psychiatric disorders: insomnia, libido decreased, restlessness.
Reproductive system and breast disorders: amenorrhea, breast discharge, breast enlargement/breast swelling, breast tenderness/breast pain, ejaculation disorder, erectile dysfunction, galactorrhea, gynecomastia, menstrual disorder, menstruation delayed, menstruation irregular, sexual dysfunction.
Respiratory, thoracic and mediastinal disorders: nasal congestion.
Skin and subcutaneous tissue disorders: drug eruption, pruritus, pruritus generalized, rash, urticaria.
Demographic Differences: An examination of population subgroups in the double-blind placebo-controlled trials did not reveal any evidence of differences in safety on the basis of age, gender, or race alone; however, there were few subjects ≥ 65 years of age and older.
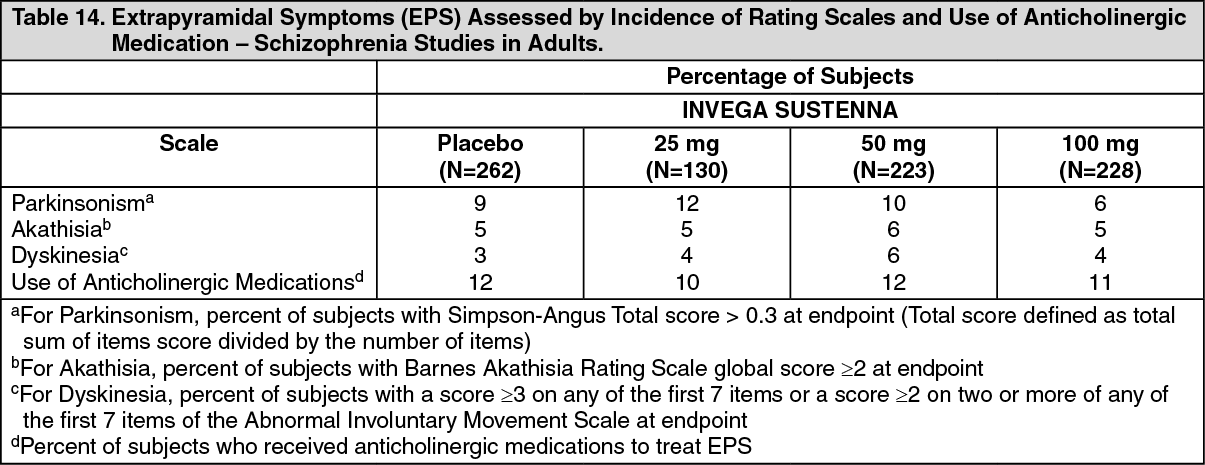
Extrapyramidal Symptoms (EPS): Pooled data from the two double-blind, placebo-controlled, 13-week, fixed-dose trials in adult subjects with schizophrenia provided information regarding EPS. Several methods were used to measure EPS: (1) the Simpson-Angus global score which broadly evaluates parkinsonism, (2) the Barnes Akathisia Rating Scale global clinical rating score which evaluates akathisia, (3) the Abnormal Involuntary Movement Scale scores which evaluates dyskinesia, and (4) use of anticholinergic medications to treat EPS (Table 14), and (5) incidence of spontaneous reports of EPS (Table 15). (See Tables 14 and 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image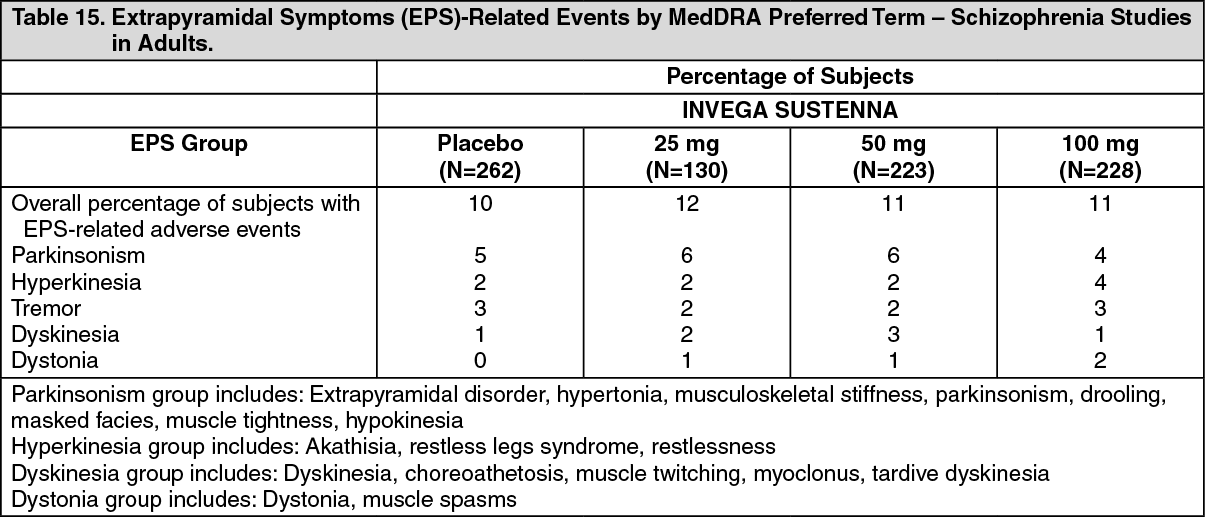 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe results across all phases of the maintenance trial in subjects with schizophrenia exhibited comparable findings. In the 9-week, fixed-dose, double-blind, placebo-controlled trial, the proportions of parkinsonism and akathisia assessed by incidence of rating scales were higher in the INVEGA SUSTENNA 100 mg group (18% and 11%, respectively) than in the INVEGA SUSTENNA 50 mg group (9% and 5%, respectively) and placebo group (7% and 4%, respectively).
In the 13-week study in subjects with schizophrenia involving 150 mg initiation dosing, the incidence of any EPS was similar to that of the placebo group (8%), but exhibited a dose-related pattern with 6%, 10%, and 11% in the INVEGA SUSTENNA 150/25 mg, 150/100 mg, and 150/150 mg groups, respectively. Hyperkinesia was the most frequent category of EPS-related adverse events in this study, and was reported at a similar rate between the placebo (4.9%) and INVEGA SUSTENNA 150/100 mg (4.8%) and 150/150 mg (5.5%) groups, but at a lower rate in the 150/25 mg group (1.3%).
In the long-term study in subjects with schizoaffective disorder, EPS reported during the 25-week open-label INVEGA SUSTENNA treatment included hyperkinesia (12.3%), parkinsonism (8.7%), tremor (3.4%), dyskinesia (2.5%), and dystonia (2.1%). During the 15-month double-blind treatment, the incidence of any EPS was similar to that of the placebo group (8.5% and 7.1% respectively). The most commonly reported treatment-emergent EPS-related adverse events (>2%) in any treatment group in the double-blind phase of the study (INVEGA SUSTENNA versus placebo) were hyperkinesia (3.7% vs. 2.9%), parkinsonism (3.0% vs. 1.8%), and tremor (1.2% vs. 2.4%).
Dystonia: Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
Pain Assessment and Local Injection Site Reactions: In the pooled data from the two 13-week, fixed-dose, double-blind, placebo-controlled trials in subjects with schizophrenia, the mean intensity of injection pain reported by subjects using a visual analog scale (0 = no pain to 100 = unbearably painful) decreased in all treatment groups from the first to the last injection (placebo: 10.9 to 9.8; 25 mg: 10.3 to 7.7; 50 mg: 10.0 to 9.2; 100 mg: 11.1 to 8.8). The results from both the 9-week, fixed-dose, double-blind, placebo-controlled trial and the double-blind phase of the maintenance trial exhibited comparable findings.
In the 13-week study involving 150 mg initiation dosing in subjects with schizophrenia, occurrences of induration, redness, or swelling, as assessed by blinded study personnel, were infrequent, generally mild, decreased over time, and similar in incidence between the INVEGA SUSTENNA and placebo groups. Investigator ratings of injection pain were similar for the placebo and INVEGA SUSTENNA groups. Investigator evaluations of the injection site after the first injection for redness, swelling, induration, and pain were rated as absent for 69-100% of subjects in both the INVEGA SUSTENNA and placebo groups. At Day 92, investigators rated absence of redness, swelling, induration, and pain in 95-100% of subjects in both the INVEGA SUSTENNA and placebo groups.
Additional Adverse Reactions Reported in Clinical Trials with Oral Paliperidone: The following is a list of additional adverse reactions that have been reported in clinical trials with oral paliperidone: Cardiac disorders: bundle branch block left, sinus arrhythmia.
Gastrointestinal disorders: abdominal pain, small intestinal obstruction.
General disorders and administration site conditions: edema, edema peripheral.
Immune system disorders: anaphylactic reaction.
Infections and infestations: rhinitis.
Musculoskeletal and connective tissue disorders: musculoskeletal pain, torticollis, trismus.
Nervous system disorders: grand mal convulsion, parkinsonian gait, transient ischemic attack.
Psychiatric disorders: sleep disorder.
Reproductive system and breast disorders: breast engorgement.
Respiratory, thoracic and mediastinal disorders: pharyngolaryngeal pain, pneumonia aspiration.
Skin and subcutaneous tissue disorders: rash papular.
Vascular disorders: hypotension, ischemia.
Postmarketing Experience: The following adverse reactions have been identified during postapproval use of paliperidone; because these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure: angioedema, ileus, swollen tongue, thrombotic thrombocytopenic purpura, urinary incontinence, and urinary retention.
Cases of anaphylactic reaction after injection with INVEGA SUSTENNA have been reported during postmarketing experience in patients who have previously tolerated oral risperidone or oral paliperidone.
Paliperidone is the major active metabolite of risperidone. Adverse reactions reported with oral risperidone and risperidone long-acting injection can be found in the Adverse Reactions sections of the package inserts for those products.
View ADR Monitoring Form